The turnover rate for long-term care nurses is far higher than the national average, but facilities can improve retention by adjusting human resources practices, a top workforce researcher said in a McKnight’s webcast Thursday.
While it is no secret that long-term care operators see high turnover rates, the hard numbers show just how serious the issue is, said Frederick Morgeson, Ph.D., of Michigan State University. The national turnover rate for all professions is about 4.5 years, while the rate for registered nurses in long-term care is about a year, according to Morgeson. Organizations with 150 nurses could face between $1.25 million to $2 million a year in the costs of losing nurses, he said.
Providers should consider the recruitment messages they are sending and how these can sow the seeds of future turnover, he said. For example, if a job posting promises opportunities for relocation or career advancement, this could effectively address nurses’ desire for professional growth — the lack of which they often cite as a source of dissatisfaction, according to Morgeson. However, if a provider cannot actually deliver on this promise, the company is likely to attract and hire an applicant who will go on to be unhappy and leave the job.
Designation as a board-certified nurse is the ultimate credential for high-quality nursing. Join 500 of your dedicated nursing colleagues at the ANCC Board Certification Nursing Conference to renew that commitment to nursing excellence.
Up to 14.5 contact hours
Top 3 Reasons to Attend:
Connect With Peers—Network with your certified nurse peers.
Commit to Professional Growth—Participate in hands-on sessions led by experts in your field.
Excel at Patient Care—Meet the highest standards of excellence and continue delivering high-quality health care.
Conference Highlights:
Earn CEs for renewal—including pharmacology!
Learn about clinical and professional best practices in nursing that you can implement right away.
Hear about new trends in nursing’s healthcare services and technologies.
Choose from two educational tracks—clinical or professional/business.
Register now to ensure you gain the knowledge and skills necessary to maintain your certification and deliver advanced patient care.
The ANCC Board Certification Nursing Conference will also be celebrating Certified Nurses Day (March 19th) and the 40th anniversary of the ANCC Certification Program.
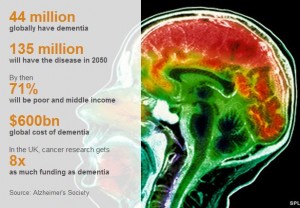
The NY Times didn’t cover it; neither did the Washington Post or the Wall Street Journal. But the BBC made a big deal of the G8 “dementia summit,” hosted by the UK just a month ago. Representatives from the research world, the pharmaceutical industry, and the Organization of Economic Development, along with government health leaders, met to discuss what to do about Dementia.
Almost all the members of the G8 took the conference seriously: the UK, Canada, France, Germany, Italy, Japan, and Russia each sent their top health representative. The US didn’t send the Secretary of Health and Human Services or an assistant secretary. The US sent the “acting assistant secretary for planning and evaluation” in the Department of Health and Human Services. This says it all: the US didn’t regard this conference as a priority.
What is Dementia?
It is an umbrella term that describes about 100 diseases in which brain cells die on a huge scale.
All damage memory, language, mental agility, understanding and judgement.
Alzheimer’s disease is the most common form, affecting 62% of those living with dementia.
It gets worse with time and eventually people are left completely dependent on carers.
From both an individual and a public health perspective, frailty is one of the most important conditions affecting older people. Along with dementia, which is really just cognitive as opposed to physical frailty, it is a devastating syndrome. Frailty predisposes to recurrent hospitalizations and leads to the dreaded cascade of iatrogenic complications once someone is in the hospital. Frailty leads to nursing home placement and to disability and death. So a recent consensus statement discussing how to approach frailty is one of the most exciting and significant papers to appear in the recent geriatric literature. Published in a third tier medical journal, it’s only by chance that I stumbled on the article at all.
No one wants to be labeled “frail.” It’s up there along with “elderly” or “old” as a term everyone seems to want to avoid. But far better to prevent or treat the condition than to pretend it doesn’t exist. It’s time for doctors to pay attention to frailty—to recognize when it’s present and to intervene when possible. How’s that for a New Year’s Resolution!
Webinar for Journalists – “How the Affordable Care Act Affects Baby Boomers and Medicare Beneficiaries” presented by the Kaiser Family Foundation’s Media Fellowships Program.
Featuring two Kaiser Family Foundation experts, the webinar began with brief presentations of the major changes for older people. Senior Fellow Karen Pollitz focused on the ACA’s role for baby boomers who are not yet 65 and eligible for Medicare and their access to new coverage options in marketplaces and/or their eligibility for premium subsidies or Medicaid expansions. Associate Director of the Program on Medicare Policy Juliette Cubanski talked about how the ACA impacts Medicare benefits and beneficiaries. We also touched on some of the major open enrollment issues for both Obamacare and Medicare. Most of the hour was devoted to a question and answer session with the participating audience.
Pressure ulcers – commonly called bedsores — are a big problem in the United States. More than 2.5 million U.S. residents develop pressure ulcers every year, with about 60,000 people dying each year from pressure ulcer complications.
Today is International Stop Pressure Ulcer Day, a day dedicated to bringing awareness to the causes and ways to prevent pressure ulcers.
“This is not just a problem for patients and their families, but also health facilities,” said Joyce Black, Ph.D., associate professor in UNMC’s College of Nursing, who is recognized as a national expert in pressure ulcers. “The government won’t reimburse for Medicare and Medicaid expenses if patients get pressure sores.”
Pressure ulcers can develop in as little as three hours as a result of sitting or lying too long in the same position, she said. Those who are bedridden are most at risk, including those in hospitals and long term care facilities like nursing homes. It can happen in the home as well.
“Ulcers develop quickly depending on how hard the surface is that you’re on and how much fat padding a person has,” Dr. Black said. “Thin, frail individuals develop them more quickly.”
She said pressure ulcers develop due to pressure on the soft tissues when patients don’t move or continuously slide down in a chair. The blood in the area stops and the tissue dies. Most problems with ulcers occur on the buttocks, tailbone and the heel of the foot.
Tips on prevention and treatment
Dr. Black has these tips for preventing and treating minor pressure ulcers.
Sit or lay in different position, walk if you can.
Stay off the sore spot until the pain or red or purple color goes away.
Put a pillow under the calf of the leg to keep the heel off of the bed.
Don’t rub the skin. It may tear.
Keep skin clean. The healthier you can keep skin the less chance of skin breakdown.
Make sure diapers get changed.
Turn individuals every three hours if they are on a good mattress. Every two hours if mattress is thin, frayed or worn.
Cover wound with dressing or apply topical antibiotic to keep wound clean.
Ask what the facility is doing to reduce or prevent bed sores and if you can help.
Ask how they are turning your loved one to get them off their back (individual should be turned on their sides-family members can help).
Ask what kind of mattress the patient is sleeping on. An old spring mattress with an inch padding is not adequate. Family may be well advised to go to a bedding store and get two inches of memory foam so there is more padding on the bed.
Make sure the patient is eating a well-balanced meal (not junk food).
The 1.4 million people who live in nursing homes are among the most vulnerable, powerless individuals in American society. They are old (mean age 79.2), they are physically frail (60% are unable to do 4 or more of the most basic daily activities), and most of them are cognitively impaired, many of them severely (39%). Nursing homes have come a long way since the bad old days when residents were tied up, neglected, and abused, and one of the stratagems for improving care has been the “care planning meeting.” A plan of care must be developed by the facility staff for all new admissions to nursing homes that are Medicare or Medicaid certified, addressing physical, emotional, and medical needs. These plans are reviewed on a quarterly basis—more often if there is a major change in status, such as a hospitalization. And one of the innovations of the last decade is to invite family members to participate in care planning meetings. This gives families information about their loved one and an opportunity to make suggestions and raise concerns. But one issue that neither staff nor families routinely raise and that the many websites that advise families about how to negotiate the unfamiliar nursing home terrain is medications. And that, specially in light of recent revelations, is an essential question.
The recent revelation is that Johnson & Johnson, the world’s largest drug company, just settled a variety of civil and criminal complaints about its sales of the psychiatric drug Risperidone (Risperdal) for $2.2 billion (yes, that’s billion) J&J “accepted accountability” for misbranding Risperdal as useful for treating elderly patients with dementia, for marketing Risperdal for the elderly, and for paying kickbacks to both physicians and to Omnicare, the largest pharmacy supplying nursing homes, for using the drug.
Since the 1990s, physicians and patients have been fighting over futility. The doctors look at a patient who is dying and say that further tests and treatment cannot possibly work and shouldn’t be done. The patients, or more commonly their families, look at those same patients and say that they want “everything done” to try to prolong life.
As often happens in the US, the futility battle ended up in the court room. In the case of Helga Wanglie, an 86-year-old woman in a vegetative state after hip surgery, the doctors went to court over whether the patient’s husband had the right to insist that she remain on a ventilator. The court, as also often happens, didn’t address the issue of whether the ventilator was or was not appropriate treatment for Mrs. Wanglie; it simply ruled that her husband, as her surrogate, had the right to make the decision. After that case, many physicians concluded that the fight over futility was itself futile. For the last 15 years, physicians have tried to focus on determining a patient’s goals of care and then suggesting what treatments are most consistent with those goals. When they still cannot agree with family members about the right course of action, they resort to mediation, sometimes provided by a hospital ethics committee. But simmering below the surface, conflicts over perceived futility rage bubble vigorously.
A short article in the New England Journal of Medicine, “The Debt of Life—Thai Lessons on a Process-Oriented Ethical Logic,” offers a refreshing way of looking at futility. Based on his experiences doing ethnographic field work in Thailand while a graduate student in Anthropology, physician Scott Stonington shines a new light on the typical ICU dilemma. The physicians, he reports, are loathe to perform various possible tests and treatments because they think in terms of outcomes. They argue that their interventions won’t work in the sense that they won’t overcome the existing medical problems and that they are burdensome to the patient and, parenthetically, expensive. The patient’s family, he observes, think in terms of the process of care. He comments on one Thai family who said that their father had given them “flesh, blood, and breath” so they had a “debt of life” to pay. The ICU, they reasoned, allowed them to repay their debt: it gave their father flesh (tube feedings for nutrition), blood (intravenous medications and dialysis to cleanse the blood), and breath (a ventilator for breathing). The family was not so much interested in the outcome of treatment as in the treatment itself. In this scenario, the conflict was ultimately resolved when the family came to the conclusion that they had paid their debt and further aggressive care could be discontinued.
I made a very similar argument in my essay, “The Standard of Caring: Why Do We Still Use Feeding Tubes in Patients with Advanced Dementia?” I noted that it had been over 10 years since a series of studies in the medical literature reported that feeding tubes (a tube inserted into the stomach to provide nutrition) did not prolong life in patients with advanced dementia who had eating difficulties. These patients are nearing the end of their lives and no matter what procedures they have, their prognosis remains pretty much the same. Not only don’t the tubes prolong life, but they don’t accomplish a variety of other goals that doctors had hoped they might: preventing pressure ulcers (skin breakdown that is often related to malnutrition) or preventing pneumonia (caused by food going into the lungs instead of the stomach). As a result of these studies, the rate of tube feeding people with advanced dementia has declined, but it is still far from zero. I suggest that the reason some families want a feeding tube is to show that they care. It’s not that they expect to improve some quantifiable outcome—living longer or avoiding pneumonia. It’s that they want to have a way to demonstrate caring. For the same reason, we keep people with advanced dementia clean and dressed. We don’t require a study that shows that they will be less likely to develop an infection if they are kept clean. We don’t demand proof that they will live longer if they are clothed. We assume that being clean and clothed contribute to well-being because they are among the only ways we as caregivers have of showing respect for the human being who happens to have dementia. Tube feeding, from this perspective, is a means of proving that we care.